Analysis of FY 2021 HRSA 340B Covered Entity Audits

Lindsay Bealor Greenleaf, JD, MBA
February 23, 2023
ADVI Health analyzed HRSA’s FY 2021 covered entity final audit results to assess covered entity compliance.[vi] ADVI analyzed the audit findings at the national and state levels. ADVI found the following: More than 60 percent of audited covered entities at had least one adverse finding (referred to in this analysis as a “non-compliant covered entity”); Nearly 30 percent (37 of 124) of non-compliant covered entities had two or more adverse findings; and At the state level, the highest number of covered entities audited in a single state was 17, while zero covered entities were audited in 5 states.
Since the 340B Drug Pricing Program began in 1992, covered entities’ participation has been contingent on compliance with statutory program requirements.
In fiscal year (FY) 2012, Health Resources and Services Administration (HRSA) began conducting audits of covered entities.[1] In 2012, sales at the 340B price totaled $6.9B.[2] In 2021 (the most recent data available), sales at the 340B price reached a record $43.9B.[3] This represents an average annual increase of almost 23 percent between 2012 and 2021.[4] The number of covered entity sites experienced dramatic growth, increasing from less than 20,000 covered entity sites in 2012 to more than 50,000 in 2023.[5] Despite this growth, HRSA has continued to audit around 200 covered entities per year since FY 2015.[6]
ADVI Health analyzed HRSA’s FY 2021 covered entity final audit results to assess covered entity compliance.[7] ADVI analyzed the audit findings at the national and state levels. ADVI found the following:
- More than 60 percent of audited covered entities had at least one adverse finding (referred to in this analysis as a “non-compliant covered entity”)
- Nearly 30 percent (37 of 124) of non-compliant covered entities had two or more adverse findings
- At the state level, the highest number of covered entities audited in a single state was 17, while five states had zero covered entities audited [8]
HRSA’s audits focus on several areas of covered entity compliance, including 340B/Medicaid duplicate discounts,[9] medicine diversion,[10] and data submission and reporting errors and inaccuracies.
It should be acknowledged that it is not clear what standards HRSA and its audit contractors are currently using to assess covered entity compliance. Following a legal challenge in 2019, HRSA “concluded that in the absence of binding and enforceable regulations, the agency would no longer issue findings based solely on noncompliance with guidance.”[11]
This determination has far-reaching implications for 340B program integrity. As a result of this policy change, HRSA stated there were 36 instances during its FY 2019 audits that did not result in a finding of noncompliance but would have resulted in one in the past.[12] The lack of clarity around program requirements and limited oversight has been well documented by the Government Accountability Organization (GAO), which has previously stated that “HRSA’s oversight of the 340B program is inadequate.”[13]
Despite these significant limitations on HRSA’s audit capabilities, ADVI’s analysis still found 62 percent of covered entities audited by HRSA in FY 2021 were non-compliant. The most common sanction imposed on these covered entities was a requirement that they repay affected manufacturers’ discounts for which the covered entities were not eligible. Covered entities were not required to pay penalties, nor did HRSA terminate any covered entities from the 340B program, as a result of noncompliance identified during these audits.
The following tables break out ADVI’s analysis of HRSA’s FY 2021 audit results on a national and state level.
Table 1: ADVI’s Analysis of National Level FY 2021 HRSA Audit Results

*Covered entities can have more than one adverse finding
Table 2: ADVI’s Analysis of State Level FY 2021 HRSA Audit Results and 2023 340B Covered Entity Registrations
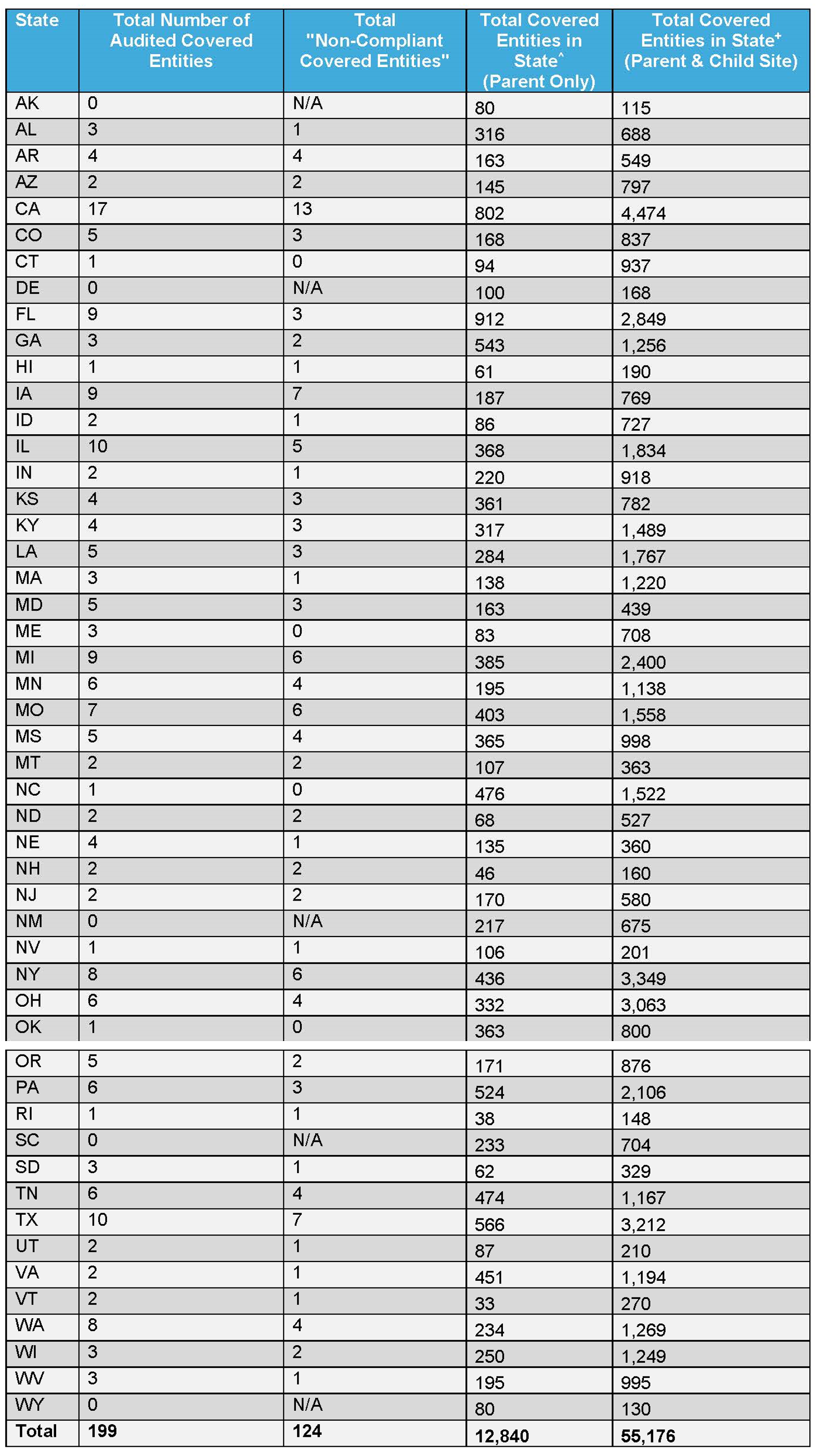
^ADVI analysis of the HRSA Office of Pharmacy Affairs (OPA) Database, 340B covered entities participating as of 1/31/2023. Analysis is at the parent level, identified based on “340B ID.” Does not take into account registrations/de-registrations throughout a year.
+ADVI analysis of the HRSA Office of Pharmacy Affairs (OPA) Database, 340B covered entities participating as of 1/31/2023. Analysis is at the individual site level (includes parent and child sites), identified based on “340B ID.” Does not take into account registrations/de-registrations throughout a year.
Funding for this research was provided by Pharmaceutical Research and Manufacturers of America. ADVI Health retained full editorial control.
Lindsay Bealor Greenleaf, JD, MBA
Senior Vice President, Market Access and Policy Strategy
CEO insights
Related articles
Real analysis from people who’ve been there

The 2026 Rare Disease Reality
Orphan drugs now represent approximately 20 percent of total prescription spend, and over 52 percent of the cell and gene …

Marc Samuels, JD, MPH
February 26, 2026

AI in the Patient Care Paradigm: Examining Regulatory Challenges to Clinical Adoption
Artificial intelligence could transform clinical care, but regulatory hurdles slow adoption. Ensuring healthcare AI has adequate policy safeguards is paramount …
Marc Samuels, JD, MPH
December 30, 2025

2026 Life Sciences Forecast: AI, Next-Gen Cell & Gene Therapy, and Policy Disruption
In 2026, we expect the healthcare landscape to be defined by technology breakthroughs, market access disruption, and profound policy changes. …
Marc Samuels, JD, MPH
December 16, 2025

Delivering on CAR T-cell Therapy’s Promise: Policy Solutions for the Next Era of Cancer Care
CAR T-cell therapy offers a groundbreaking treatment option for patients with relapsed or refractory hematologic malignancies, yet access remains severely …

Alicia Silver, MPP
November 21, 2025
Why is Medicare Data Central to IRA Negotiations?
The Inflation Reduction Act (IRA), passed in 2022, has transformed the way drug pricing will be managed in the United …

The Unintended Consequences of Drug Pricing Policies on Orphan Drug Development
Rare diseases impact nearly 1 in 10 people in the US and are largely untreated, with 95 percent lacking FDA-approved …

Tyler Seville, MPA
June 23, 2025

ADVI Analysis: HRSA 340B Covered Entity Audits
Analysis of HRSA 340B Covered Entity Audits Since the 340B Drug Pricing Program began in 1992, covered entities’ participation has …

Prescription Drug Affordability Boards: Access Concerns and Implications for Rare Diseases and Conditions
In recent years, states have increasingly enacted Prescription Drug Affordability Boards (PDABs). While their stated purpose is to increase affordability, …

Allison Schneider, MHA
February 28, 2025
Reach out
Own your edge
We don’t just guide the market. We shape it. Map your market access moves with #ADVIIntelligence. Proven advantage. Unmatched partnership.