ADVI Instant: CMS Finalizes Guidance on IPAY 2027 Negotiation and MFP Implementation for 2026/27

Lindsay Bealor Greenleaf, JD, MBA
October 11, 2024
On October 2, 2024, CMS issued final guidance on the Medicare Drug Price Negotiation Program for IPAY 2027 and Manufacturer Effectuation of the Maximum Fair Price (MFP) in 2026 and 2027 (link).
Notable highlights from the final guidance include:
- A roundtable and town hall approach to public engagement that replaces the IPAY 2026 patient-focused listening sessions
- A revised negotiation process which provides optional meetings and additional written offers/counteroffers
- Details on the two functions of the yet to be announced Medicare Transaction Facilitator (MTF) contractor(s), the data module and payment module
- Information on forthcoming dispensing entity requirements for MFP effectuation
Changes to the Selection and Negotiation Process
Selection
- CMS made few substantive changes to the process of selecting drugs for negotiation.
- As proposed in draft guidance, CMS notes the following:
- Low-Spend Medicare Drug Exclusion: CMS will apportion Part B expenditures for drugs that map to the same HCPCS based on the ratio of reported sales volume of a drug compared to all drugs.
- Deadline to apply for IPAY 2027 Small Biotech Exception and Initial Biosimilar Delay: “mid-December 2024.”
- Small Biotech Exception and Acquisitions: CMS will evaluate whether Submitting Manufacturers were acquired before January 1, 2025.
- Bona Fide Marketing of generic/biosimilar: CMS will apply a similar approach as IPAY 2026 selection.
- ADVI Note: CMS maintains that it will check for bona fide marketing by reviewing PDE & AMP data through January 15, 2025. This is notable as there has been speculation that CMS might release the IPAY 2027 list well in advance of the February 1, 2025 statutory deadline (as early as December 2024) if Trump wins the election.
- In final guidance, CMS added the following:
- It will identify the active moiety or ingredient of the drug using RxNorm, OpenFDA, FDALabel, and FDA’s Active Ingredient-Active Moiety Relationship/Basis of Strength file.
- The NDC Directory’s NDC Excluded Drugs Database file will be included as a source that CMS will use to identify NDC-11s of the selected drug.
Public Submissions
- As proposed in draft guidance, CMS is grouping questions by category of respondent (e.g., manufacturer input, patient or caregiver experience, clinical experience, health research) to align information with a respondent’s area of expertise.
- CMS also revised questions within the categories, including a request of a description about “what it is like to live with a medical condition treated by the selected drug or its therapeutic alternative(s)” and “the factors a patient cares about most when assessing the value of a drug”
- CMS notes that despite groupings, stakeholders can answer any question.
Manufacturer Submissions
- As proposed in draft guidance, CMS made the following changes:
- Will require several new data elements to be submitted by manufacturers, including drug-level data on samples, labeler codes, private labeler distributors, and units per package.
- Revised definitions of some submission elements, which clarified the following:
- Transfer prices should not be included in current unit costs of production
- R&D pre-clinical costs should be limited to FDA-approved indications; CMS adds a new category to capture R&D related to failed and abandoned products, non-approved indications
- Coupons should be excluded from US commercial average net unit price – net of patient assistance programs, but not US commercial average net unit price
- Off-label use means a use not approved by the FDA but “is included in nationally recognized, evidence-based guidelines and listed in CMS-recognized Part D compendia”.
- In final guidance, CMS made the following additional changes:
- Revised the previously proposed data element (new to the IPAY 2027 draft guidance) “Manufacturer net Medicare Part D Price” to “Manufacturer net Medicare Part D average unit Price”
- The element would include “specific data, including coverage gap discounts and other supply chain concessions (e.g., wholesale discounts) of the Primary Manufacturer or any Secondary Manufacturer(s) not reflected in the sum of the plan-specific enrollment weighted amounts calculation, and utilization that may differ from the PDE data”
- Added a new data element “Manufacturer net Medicare Part D average unit price – best”, which is defined as “the lowest manufacturer net Medicare Part D average unit price offered by the Primary Manufacturer or any Secondary Manufacturer(s) to any Part D plan sponsors in the U.S.”
- The element would include “specific data, including coverage gap discounts and other supply chain concessions (e.g., wholesale discounts) of the Primary Manufacturer or any Secondary Manufacturer(s) not reflected in the sum of the plan-specific enrollment weighted amounts calculation, and utilization that may differ from the PDE data”
- Added “costs associated with generating real-world evidence” to the definition of “Other Direct R&D Costs”
- Noted that “prior federal financial support” includes manufacturers’ reasonable estimate of the dollar value of in-kind contributions and Cooperative Research and Development Agreements (CRADAs) that do not have a readily ascertainable value
- Added more detail (e.g., examples) to the definitions of patent and patent applications and noted that relevant patents do not include applications denied by the USPTO
- Revised the definition of therapeutic advance note that:
- Therapeutic advance will be determined in comparison to therapeutic alternatives and by examining the extent to which the selected drug provides a substantial improvement in outcomes for an indication(s)
- Note: CMS will consider the extent to which a selected drug represents a therapeutic advance at the time of submission of the Negotiation Data Elements and Drug Price Negotiation ICR
- Therapeutic advance will be determined in comparison to therapeutic alternatives and by examining the extent to which the selected drug provides a substantial improvement in outcomes for an indication(s)
- Revised the previously proposed data element (new to the IPAY 2027 draft guidance) “Manufacturer net Medicare Part D Price” to “Manufacturer net Medicare Part D average unit Price”
- Other changes to the manufacturer submission process include:
- CMS added the NDC Directory as an additional source that the agency will use to populate NDC-11s in the CMS HPMS system
- In advance of publishing the statutorily required explanation of the MFP by March 1, 2026, CMS states that it may share “aggregate or non-selected drug specific information”, for instance, on the status of the negotiation process
Public Engagement Opportunities
- After noting its intention to revise the patient-focused listening sessions for IPAY 2027 in draft guidance, CMS will offer closed-door patient-focused roundtables and a public town hall.
- Spring 2025: CMS intends to host up to 15 patient-focused roundtable events that will feature a discussion-based format instead of a listen-only format.
- These events will be held virtually but not livestreamed and limited to patients, patient advocacy groups, and caregivers, however a redacted transcript will be published for each event.
- These events will “aggregate” selected drugs by condition when appropriate
- CMS will also host one town hall meeting in Spring 2025 focused on clinical considerations related to selected drugs.
- CMS encourages participation from clinicians and researchers, however it will be available to the public and livestreamed.
- Spring 2025: CMS intends to host up to 15 patient-focused roundtable events that will feature a discussion-based format instead of a listen-only format.
- For both events, CMS will use an “intentional process” to select speakers.
MFP Final Offers
- As proposed in the draft guidance, CMS’s starting point for initial offers for IPAY 2027 will be based on a therapeutic alternative’s Net Part D Plan Payment and Beneficiary Liability and/or the ASP, or its MFP, if applicable.
- Net Part D Plan Payment and Beneficiary Liability is defined as the Part D total gross covered drug cost net of DIR and Coverage Gap Discount Payments.
- In the Final Guidance, CMS notes that it will exclude PDE records from the above calculation for which a compound code indicates the PDE record is for a compounded drug.
- Note: in IPAY 2026, the starting point price was the Part D price net of all price concessions in DIR.
- Net Part D Plan Payment and Beneficiary Liability is defined as the Part D total gross covered drug cost net of DIR and Coverage Gap Discount Payments.
Negotiation Process
- CMS acknowledges that the IPAY 2027 negotiation period is one month shorter than the IPAY 2026 negotiation period (per the statute) and is accordingly making timeline adjustments.
- For information on the ceiling price and calculation of a single MFP:
- CMS will provide within 45 days (instead of 60 days as for IPAY 2026),
- Manufacturers may respond with suggestions of error within 21 days (instead of 30 days as for IPAY 2026), and
- CMS will respond, if feasible, within 21 days (instead of 30 days as for IPAY 2026).
- For negotiation meetings:
- In draft guidance, CMS noted it may reduce the number of negotiation meetings or replace meetings with additional written offer opportunities.
- In the final guidance, CMS outlines a revised process for up to 3 optional meetings and “additional price exchange opportunities”:
- CMS will reach out to the manufacturer and offer to hold an optional negotiation meeting after the initial offer is issued but before the counteroffer is due.
- CMS states that this meeting would likely focus on the evidence CMS used to develop the initial offer for the MFP but would not be limited to this topic.
- While CMS may discuss oral counteroffers during the meeting, such offers will not be accepted as CMS intends to respond to statutory written counteroffers in writing as obligated.
- If a Primary Manufacturer declines the first optional meeting, CMS will not increase the number of total meetings in the negotiation process.
- The Primary Manufacturer and CMS may conduct up to two additional meetings if CMS rejects the Primary Manufacturer’s written counteroffer.
- CMS will reach out to the manufacturer and offer to hold an optional negotiation meeting after the initial offer is issued but before the counteroffer is due.
- CMS will also offer an optional negotiation meeting to manufacturers if it rejects the written counteroffer, and if MFP agreement is not reached in that meeting, it will offer another, final, optional meeting.
- This process reflects a change from IPAY 2026 where each party (i.e., manufacturers or CMS) could request additional meetings, only after the statutory written counteroffer
- “Additional Price Exchange Opportunities” in Writing
- New in final guidance, “additional price exchange opportunities” will allow CMS and manufacturers to exchange additional, written offers and counteroffers.
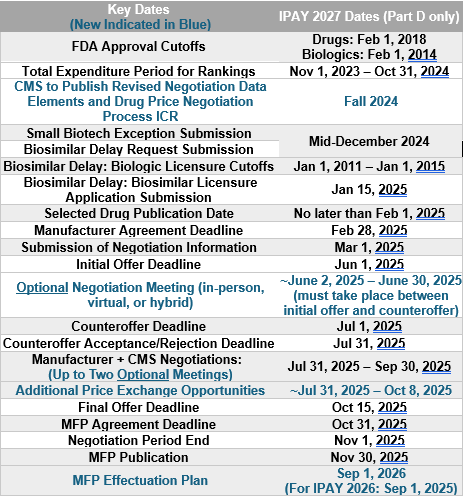
- The additional written offers may take place after CMS’ rejection of the initial, statutory written counteroffer (no later than July 31, 2025), and one week before final offers must be sent my CMS (October 8, 2025).
- The additional price exchange opportunities do not replace optional negotiation meetings, rather the negotiation meetings may be used to discuss justifications for offers/counteroffers.
- These offers will be exchanged via HPMS and will include optional text fields for additional, contextual information.
- For information on the ceiling price and calculation of a single MFP:
Timeline
Implementation of the MFP
Medicare Transaction Facilitator (MTF) Functions: Data and Payment Modules
- CMS confirms it will engage an MTF Contractor (or contractors) to facilitate the exchange of data and payment between Primary Manufacturers (herein referred to as manufacturers) and dispensing entities
- CMS distinguishes MTF functions into the Data Module (MTF DM) and the Payment Module (MTF PM) and indicates it has initiated the acquisition process for both.
MTF Data Module - The MTF DM will perform the functions proposed in draft guidance (the collection and transmission of certain claim-level data to manufacturers, and receipt of payment information from manufacturers), as well as provide documentation of electronic (ERA) or paper payment remittance to dispensing entities for payments that pass through the MTF PM
- Participation in the MTF DM remains mandatory for manufacturers, and though CMS notes “dispensing entity participation in the MTF DM is needed”, that requirement will be addressed in future rulemaking
- CMS intends to propose requiring Part D plan sponsors to include in their pharmacy agreements provisions requiring dispensing entities to enroll in the MTF DM
- CMS will require dispensing entities to execute agreements during the MTF DM enrollment process, which will include provisions regarding data use, privacy, and security requirements
- The MTF will transmit all PDE data elements included in draft guidance, as well as “Prescriber ID” and “Prescriber ID Qualifier”.
- These fields reflect the National Provider Identifier (NPI), or other identifier of the prescriber which CMS notes may be useful “although not sufficient” for 340B nonduplication efforts
- CMS notes that it may add additional claim-level payment elements in the future
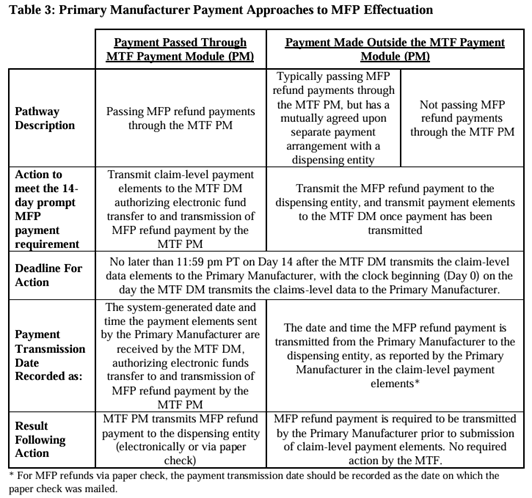
- Positive “clarification” for manufacturers: CMS is clarifying that the 14-day prompt MFP payment window begins when the MTF DM transmits claims-level data to manufacturers and is considered met if the manufacturer provides confirmation of the transmission an MFP refund within 14 days, as opposed to ensuring that the dispensing entity has received an MFP reimbursement within that timeframe. Specifics of how manufacturers can meet the MFP effectuation prompt pay requirements are detailed in new Table 3 in final guidance
- CMS received feedback from pharmacies that the 14-day prompt MFP payment window may create cashflow problems for certain dispensing entities.
- CMS believes this will only be an issue at the start of initial price applicability years (e.g., January 2026), and will resolve once refunds are “flowing.”
- To accommodate these concerns, CMS will ask dispensing entities to self-identify whether they anticipate “material cashflow concerns”. CMS expects this may include:
- Sole proprietor rural and urban pharmacies with high volume of Medicare Part D prescriptions dispensed
- Pharmacies who predominantly rely on prescription revenue to maintain business operations
- Long-term care pharmacies
- 340B covered entities with in-house pharmacies
- Indian Health Service, Tribal, and Urban Indian (I/T/U) pharmacies
- This information (i.e., a list of dispensing entities that have self-identified as anticipating material cashflow challenges) will be provided to manufacturers to assist in the development of MFP effectuation plans
- CMS notes it will develop a “flexible, efficient enrollment process” for the MTF DM to maintain dispensing entity banking information for the purpose of facilitating ERA or remittances, whether manufacturers opt to pass payment through the MTF PM or an outside arrangement
- CMS plans to allow manufacturers to view dispensing entity information in the MTF portal to facilitate payments made outside of the MTF PM, which will include a dispensing entity’s preference for how to receive payments (e.g., electronic or paper, through a third-party vendor, etc.)
- The MTF PM will transmit payments according to dispensing entities’ preferences, and manufacturers making payments outside the MTF PM must adhere to preferences as well
- An MTF ICR will be published for public comment in Fall 2024 with details on information that dispensing entities will be required to provide.
- CMS is evaluating data privacy and security implications of collecting, holding, and sharing financial information
MTF Payment Module (MTF PM)
- The MTF PM will serve the function described as “Option 2: MTF Pass Through of Primary Manufacturer Funds to Dispensing Entities” in the draft guidance.
- The MTF PM will collect banking information from dispensing entities as well as aggregated refund amounts from manufacturers and will transmit payment to the dispensing entities on behalf of manufacturers. CMS will bear the costs of operationalization of this MTF PM function, and the MTF PM will retain payment records.
- CMS stresses repeatedly that:
- Neither CMS nor its MTF Contractors will determine the payment amounts transferred through the MTF PM; and
- The MFT PM’s transfer of a refund payment to a dispensing entity does not in any way imply CMS or MTF approval of the amount paid.
- Specifically, the MTF PM will:
- Provide manufacturers with a mechanism for electronic transfer of funds or payment by paper check to facilitate MFP refund payments to dispensing entities; and
- Provide manufacturers with a credit/debit ledger system to track the flow of MFP refunds and to handle reversals, adjustments, and other claim revisions.
- While use of the MTF PM is voluntary, CMS expects most manufacturers to use this method. CMS notes that if a manufacturer elects to use the MTF PM, it will participate for all its selected drugs and typically with all dispensing entities.
- However, CMS notes that participation with the MTF PM does not preclude manufacturers from establishing MFP effectuation processes outside the MTF PM with dispensing entities.
- Manufacturers may choose to delegate MTF PM related responsibilities to a third party, but CMS notes that the manufacturer is ultimately responsible for providing timely access to the MFP.
- If the manufacturer chooses to not pass payment through the MTF PM, the manufacturer must describe the details of their approach to MFP effectuation outside of the MTF PM, including any specific arrangements with dispensing entities outside of the MTF, in its MFP effectuation plans.
Standard Default Refund Amount (SDRA)
- As previously detailed, manufacturers may make the MFP available prospectively at the time of acquisition or retroactively through a refund.
- The MTF DM will calculate a SDRA equal to:
- WAC per unit on the claim’s date of service minus MFP per unit on the claim’s date of service, multiplied by the quantity dispensed
- Note: Draft guidance did not define the SDRA at a per unit level
- Manufacturers may refund an amount different than the SDRA if they determine another amount is “appropriate and sufficient” to make the MFP available
- Dispensing entities can work with manufacturers to establish refunds based on actual acquisition cost or an adjusted standardized pricing metric
- If manufacturers and dispensing entities agree to use a refund amount based on a “reasonable proxy” for the acquisition cost, CMS will consider that refund amount sufficient to fulfill the MFP availability obligation.
- To help dispensing entities reconcile MFP refund amounts, NCPDP will provide instruction to Part D plan sponsors on including SDRAs on all Part D claims for drugs with MFPs in effect.
- Dispensing entities will see an estimated MFP refund (equal to the SDRA calculated by plan sponsors).
- If the estimated SDRA aligns with acquisition costs, dispensing entities can create an accounts receivable.
- Dispensing entities are encouraged to remediate with manufacturers directly before utilizing the complaint and dispute system.
340B Nonduplication
- Per the statute, manufacturers are required to provide access to the MFP to 340B covered entities in a nonduplicated amount to the 340B ceiling price if the MFP is lower than the 340B ceiling price for the selected drug. Manufacturers are not required to provide access to the MFP if the 340B ceiling price is lower than the MFP.
- CMS continues to assume no responsibility for deduplicating 340B and MFP discounts, noting they intend “to provide Primary Manufacturers a process to identify applicable 340B-eligible claims through the reporting of claim-level payment elements to the MTF.”
- However, CMS states that it agrees with commenters that “limited additional information to support a Primary Manufacturer with identifying 340B-eligble claims is necessary,” and is adding the “Prescriber ID” and “Prescriber ID Qualifier modifier” elements to the list of required data elements sent by the MTF DM to the Primary Manufacturer.
- Manufacturers can decline to pay MFP refunds if the claim should be excluded based on the 340B price being lower than the MFP, but documentation will be required.
- If the MFP was made available prospectively and the 340B price is lower than MFP, manufacturers would have to provide the difference between MFP and 340B price.
- CMS states that it “continues to explore the feasibility of incorporating 340B-related transactional data” into the MTF process.
- Note: CMS explicitly notes that nothing in this guidance alters a manufacturer’s liability “for an overcharge violation and sanctions for failure to provide the 340B ceiling price to eligible entities.”
MFP Effectuation Plans
- Manufacturers must submit to CMS plans on how they will make the MFP available (either through prospective sales at or below the MFP, retrospective rebates, or a combination).
- CMS is revising the deadline for MFP Plan submission to be September 1, 2025, for IPAY 2026 selected drugs, and to be September 1, 2026, for IPAY 2027 selected drugs.
- In draft guidance, CMS proposed a June 1, 2025, submission deadline for IPAY 2026; the original submission deadline for IPAY 2026 was December 2, 2025.
- CMS is revising the deadline for MFP Plan submission to be September 1, 2025, for IPAY 2026 selected drugs, and to be September 1, 2026, for IPAY 2027 selected drugs.
- CMS plans to issue an upcoming Information Collection Request (ICR) on data that should be collected to ensure the MFP is properly effectuated.
- A combination of the draft guidance comments and the ICR comments will be used to establish a standardized method of data collection for manufacturers to follow when submitting their MFP Plans.
- CMS will conduct risk assessments of each submission, and plans with greater risk of failing to make the MFP available will be subject to increased scrutiny through monitoring and oversight.
- Among other items, manufacturers must include:
- Types of documentation kept for compliance purposes
- General plans and procedures for contacting and receiving communications from dispensing entities
- Processes for mitigating material cashflow concerns for dispensing entities (e.g., prospective purchasing agreements, accelerated MFP refund timelines)
- Process for deduplicating 340B covered units
- Whether the manufacturer will participate in the MTF PM
- If the manufacturer declines to use the MTF PM, then it is required to provide:
- Its plan to meet the 14-day prompt MFP payment window,
- Policies and procedures for determining the methodology used to calculate the amount of reimbursement due
- Confirmation that it will use an auditable generally accepted accounting principles (GAAP) system
- Confirmation that it will submit verification of reimbursement to the MTF
- Method of reconciling over- or under-payments
- Processes for creating and making available remittances for each payment
- Its plan for internal auditing to ensure all transactions effectuate the MFP
- Redacted plans will be made available to dispensing entities on the MTF user interface. CMS may release the redacted plans to interested parties (e.g., supply chain entities) upon request.
- During the negotiation period, CMS states that it will monitor manufacturer compliance and may require additional information, including recurring reporting (i.e., to show that MFP is being made available) and specific, ad hoc requests for information related to monitoring, auditing, or investigation efforts
- CMS notes that, when applicable, it will provide manufacturers a written request that includes the deadline for required information and will allow for a single deadline extension if determined to have a reasonable basis.
Complaints and Disputes
- CMS will establish an intake system for complaints and disputes related to MFP availability and technical functionality of the MTF system.
- In the final guidance, CMS specified that complaints and disputes must be submitted to CMS no later than 120 calendar days from the date of the subject of the complaint or dispute.
- CMS did not otherwise make changes to the proposed process.
- Disputes will include issues raised by manufacturers and dispensing entities related to technical aspects of the MTF process, e.g., claims potentially requiring an MFP refund.
- Complaints will include issues raised by manufacturers and dispensing entities, as well as the general public, on other issues, e.g., reports of MFP not being made available.
Part D Formulary Inclusion of Selected Drugs
- CMS will continue the formulary inclusion policies described in the revised guidance for IPAY 2026 and will not implement explicit tier placement or utilization management requirements that apply across selected drugs in all formularies for IPAY 2027.
- To monitor Medicare Part D plans’ compliance with formulary requirements, CMS will use its formulary review process to assess instances where:
- Part D sponsors place selected drugs on non-preferred tiers;
- A selected drug is placed on a higher tier than non-selected drugs within the same class;
- Part D sponsors require step therapy prior to dispensing a selected drug;
- Part D sponsors impose more restrictive utilization management for a selected drug than a non-selected drug in the same class.
- To monitor Medicare Part D plans’ compliance with formulary requirements, CMS will use its formulary review process to assess instances where:
- The agency noted “if CMS identifies that Part D sponsors are not providing beneficiaries with meaningful access to selected drugs, CMS may consider implementing new requirements for future contract years.”
ADVI will continue monitoring developments and the next steps. This is a delayed release. ADVI Instant content is distributed in real-time for retainer clients. Get in touch to learn more about how we can support your commercialization, market access, and policy needs.
Lindsay Bealor Greenleaf, JD, MBA
Senior Vice President, Market Access and Policy Strategy
CEO insights
Related articles
Real analysis from people who’ve been there

The 2026 Rare Disease Reality
Orphan drugs now represent approximately 20 percent of total prescription spend, and over 52 percent of the cell and gene …

Marc Samuels, JD, MPH
February 26, 2026

AI in the Patient Care Paradigm: Examining Regulatory Challenges to Clinical Adoption
Artificial intelligence could transform clinical care, but regulatory hurdles slow adoption. Ensuring healthcare AI has adequate policy safeguards is paramount …
Marc Samuels, JD, MPH
December 30, 2025

2026 Life Sciences Forecast: AI, Next-Gen Cell & Gene Therapy, and Policy Disruption
In 2026, we expect the healthcare landscape to be defined by technology breakthroughs, market access disruption, and profound policy changes. …
Marc Samuels, JD, MPH
December 16, 2025

What HEOR Information Does CMS Need for Drug Price Negotiations Under the IRA?
As the Inflation Reduction Act (IRA) reshapes drug pricing policy in the United States, the Centers for Medicare and Medicaid (CMS) …

Delivering on CAR T-cell Therapy’s Promise: Policy Solutions for the Next Era of Cancer Care
CAR T-cell therapy offers a groundbreaking treatment option for patients with relapsed or refractory hematologic malignancies, yet access remains severely …

Alicia Silver, MPP
November 21, 2025
Real-World Effectiveness vs Clinical Trial Efficacy in Medicare
The Inflation Reduction Act (IRA) has ushered in a new era of drug pricing negotiations in the US. For the …
Why is Medicare Data Central to IRA Negotiations?
The Inflation Reduction Act (IRA), passed in 2022, has transformed the way drug pricing will be managed in the United …
The Unintended Consequences of Drug Pricing Policies on Orphan Drug Development
Rare diseases impact nearly 1 in 10 people in the US and are largely untreated, with 95 percent lacking FDA-approved …
Reach out
Own your edge
We don’t just guide the market. We shape it. Map your market access moves with #ADVIIntelligence. Proven advantage. Unmatched partnership.