Insights,
Insights,
To be eligible for 340B, a DSH hospital must have a Medicare DSH adjustment percentage above a certain threshold, among other eligibility criteria. This adjustment percentage is determined generally by the share of low-income Medicare and Medicaid patients that receive inpatient care at a hospital. Given the DSH adjustment percentage’s importance in determining eligibility for 340B — a discount program for outpatient medicines — this study provides important context for the current policy discussions on the size and scope of the 340B program. MedPAC recently voiced concern over the appropriateness of using DSH to allocate safety net dollars as it may not efficiently identify health care facilities serving the most high-need patients, like Medicare beneficiaries with low-income subsidy (LIS) or dual Medicare/Medicaid status.i
Our study found that inpatient Medicare beneficiaries served at 340B DSH hospitals are more likely to have low-income subsidy (LIS) or dual Medicare/Medicaid status than outpatient beneficiaries receiving 340B medicines at 340B hospitals and child sites. The significant difference between Medicare beneficiary demographics for inpatient and outpatient claims demonstrates that inpatient metrics—like DSH thresholds—may not be the most appropriate measure to determine covered entity eligibility for the outpatient-based 340B drug discount program.
Results
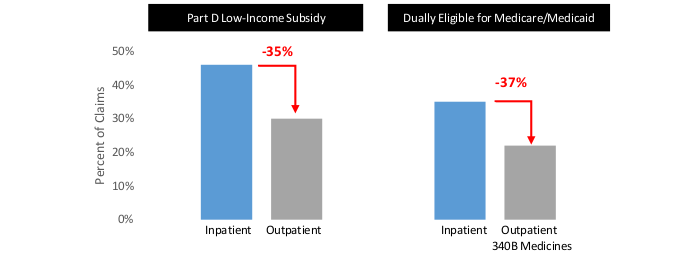
All results and data shown within this paper are for 2020, but these findings were consistent across the prior years included in the analysis. Figure 1 shows the share of the Medicare FFS population receiving care at 340B facilities with LIS and those dually eligible in Medicare/Medicaid (“duals”). Beneficiaries receiving outpatient medications through the 340B drug pricing program are approximately 35% less likely to have LIS or dual status than the percent of the population receiving inpatient care at these hospitals. This suggests patients receiving inpatient treatment are significantly more likely to be lower income than patients receiving 340B medicines in the outpatient setting.
Figure 1 – Share of Medicare Populations Receiving Care at 340B DSH Parent and Child Sites, By Indicators of Socio-Economic Status (2020)
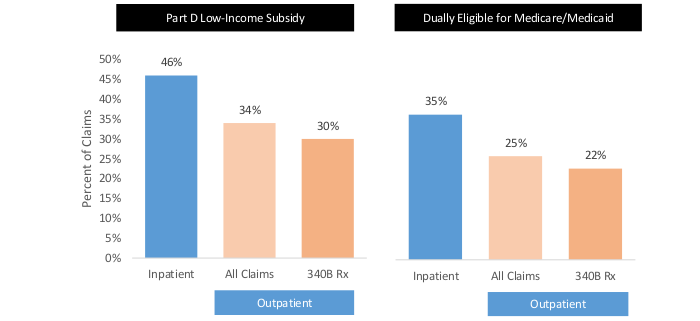
Additionally, we compared all patients receiving outpatient care and patients receiving 340B prescription medicines in the outpatient setting at the same 340B DSH hospitals and child sites. Figure 2 shows that beneficiaries receiving outpatient care are more likely to have LIS or dual status than those receiving 340B outpatient medicines. This suggests patients receiving 340B medicines are not only less likely to be lower income when compared to patients treated in the inpatient setting, but also when compared to all patients receiving treatment in the same outpatient settings.
Figure 2 – Share of Medicare Populations Receiving Care at 340B DSH Parent and Child Sites, By Indicators of Socio-Economic Status (2020)
Key Findings and Policy Implications
Inpatient Medicare FFS beneficiaries served at 340B DSH hospitals are more likely to have LIS or dual status than Medicare FFS beneficiaries receiving drugs in outpatient settings at 340B DSH hospitals and child sites. In addition, the population receiving drugs acquired through the 340B program have a smaller proportion of beneficiaries that are low income compared to the overall outpatient population at these same facilities, as indicated by a lower share of LIS and dual status beneficiaries.
The significant difference between Medicare beneficiary demographics for inpatient claims compared to outpatient claims demonstrates that inpatient metrics—like DSH thresholds—may not be the most appropriate measure to determine covered entity eligibility for the outpatient-based 340B drug discount program.
Methodology
The HRSA (Health Resources and Services Administration) online database was used to determine DSH and 340B status. Hospitals were included in the analysis if their DSH and/or 340B status was active throughout the entirety of the calendar year. The status was assigned to the Medicare Provider Number, which means that the parent site and all child sites will have the same DSH/340B status in this analysis. This DSH/340B status was then merged with the claims database (Research Identifiable Files [Inpatient and Outpatient] – 2018-2020) by the Medicare Provider Number. 340B outpatient medicines are defined as any claim that contains a drug line with HCPCS modifiers of “JG” or “TB” indicating it was purchased through the 340B drug pricing program. Non-340B drug claims are any claim for a drug that has no JG or TB HCPCS modifier. Beneficiaries with multiple claims were counted individually, which gives more weight those with multiple encounters or drug prescriptions at a particular facility.
i MedPAC. Report to Congress: Medicare and the Health Care Delivery System. June 2022.
This study was funded by Pharmaceutical Research and Manufacturers of America (PhRMA).